Study Sheds Light on Why Wounds Often Heal Poorly in Diabetics
By: Asher Jones
When tiny particles called exosomes, which shuttle signals between cells, are defective in diabetic patients, they can drive inflammation and impair healing of wounds, according to a new Nano Today study led by University of Pittsburgh and UPMC researchers.
In chronic wounds of diabetes patients, these faulty exosomes can’t deliver vital information to cells that promote wound healing, the researchers led by Dr. Subhadip Ghatak, associate professor of surgery at Pitt, found. These insights open the door to new exosome-focused therapies to promote healing of chronic wounds.
Dr. Subhadip Ghatak
“In patients with diabetes, wound healing is impaired because of excess inflammation,” said co-senior author Dr. Chandan Sen, director of the McGowan Institute for Regenerative Medicine, professor of surgery and plastic surgery at Pitt and chief scientific officer of UPMC Wound Healing Services. “Left untreated, these non-healing, or chronic, wounds can lead to limb amputations. More than 100,000 diabetes-related amputations occur in the U.S. each year, but by understanding more about wound healing and developing new therapies, our goal is to bring down this number.”
Using negative pressure bandages that gently vacuum wounds to stimulate healing, Ghatak and his team collected wound fluid from chronic wounds of 22 diabetic and 15 non-diabetic patients.
“These bandages would normally be thrown in the trash can, but wound fluid is actually a very valuable sample that reflects what’s going on throughout the wound,” said Sen, who is also the associate vice chancellor for life sciences innovation and commercialization. “For example, if the wound is infected, the fluid will carry traces of that infection.”
Dr. Chandan Sen
The researchers isolated and analyzed exosomes produced by skin cells called keratinocytes. After these particles are packed with cargo — including RNA, lipids and proteins — they are released from the cell and taken up by macrophages, immune cells that coordinate wound healing.
“If signals contained within exosomes are correct, the macrophage knows how to resolve inflammation in the wound,” explained Sen. “In diabetes, crosstalk between keratinocytes and macrophages is compromised, so macrophages keep driving inflammation and the wound can’t heal.”
Diabetic exosomes, which the researchers dubbed diaexosomes, had different contents of RNA, lipids and proteins than those from non-diabetics, suggesting that the cargo packing process is altered in diabetes.
Diabetes also compromises release and uptake of exosomes in wounds, Ghatak and his team found. The number of diaexosomes in wound fluid from diabetic patients was much lower than exosomes in non-diabetics, and macrophages took up far fewer exosomes than diaexosomes.
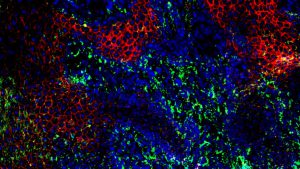
Skin cells at the edge of a diabetic wound. Red and green colors depict two proteins involved in the release of exosomes from these cells (CREDIT: Subhadip Ghatak).
When the researchers incubated non-diabetic macrophages with exosomes, the macrophages produced compounds that signify resolution of inflammation, indicating that they had received the exosome’s message and responded correctly to initiate wound healing.
But when they repeated this experiment with diaexosomes, the macrophages produced pro-inflammatory compounds common in diabetic patients with chronic wounds.
“Diaexosomes drive deviation from the healing cascade, so that resolution of inflammation is compromised,” said Sen. “And this isn’t just limited to wounds. Because exosomes are responsible for many functions in the body, diaexosomes could play a role in other diabetic complications. This study opens a new line of thinking.”
The researchers are now investigating how they could target diaexosomes to improve wound healing in diabetics. One avenue, he said, is to develop therapeutics to undo chemical modifications that occur in diaexosomes. Alternatively, they could isolate exosomes from diabetic patients and load them with missing signals before infusing them back into the wound tissue.